This chapter provides a comprehensive overview of Substance-Related and Addictive Disorders, crucial for psychology residents preparing for the In-service exam and ABPN Psychiatry Boards exam. These disorders encompass a range of conditions related to the excessive or problematic use of substances like alcohol, caffeine, cannabis, hallucinogens, inhalants, opioids, sedatives, hypnotics, anxiolytics, stimulants, and tobacco. For each substance, the chapter provides detailed information on intoxication and withdrawal symptoms, potential long-term effects, and specific treatment modalities. Additionally, non-substance-related addictions such as gambling are included due to their similar impact on the brain’s reward systems.
Authors: Minji Kwon, Brian Hanrahan MD
Editor: Christine Lagrotta, MD, Board-certified in Psychiatry and Addiction Psychiatry
Chapter Multimedia Content
Check out this chapter’s bonus multimedia content! Note, some of this content is only available to our full-access users.
Substance-Related and Addictive Disorders
- Substance-related disorders can include the following: alcohol, caffeine, cannabis, hallucinogens, inhalants, opioids, sedatives, hypnotics, anxiolytics, stimulants, and tobacco.
- Drugs taken in excess can lead to intense activation of the brain reward systems (mesolimbic pathway) by increasing dopamine levels.
- Gambling also activates the same brain reward systems.
- Long-lasting changes can occur in the reward circuits, which can cause intense cravings and multiple relapses.
- Twin studies have shown that genetics may play a role in developing substance-related disorders.
- Individuals in the age range of 18-24 years old have a relatively high prevalence of substance-related disorders.
- Involving family can reduce the drug-seeking behavior of adolescents
- Substance-related disorders are organized into two groups: substance use disorders and substance-induced disorders
Substance use disorders
- Present as continued use of the substance(s) despite significant cognitive, behavioral, and physiological symptoms.
- Substance use disorders result from chronic exposure with subsequent physical and mental dependence.
- Diagnostic items are divided into the following groups: Impaired control, social impairment, risky use, and pharmacological.
- Patients with substance use disorder must have 2 or more of the 11 symptoms below within 12 months.
- Impaired control:
- Substance is often taken in larger amounts over a longer period than was intended.
- There is a persistent desire or unsuccessful efforts to cut down or control substance use.
- A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects.
- Craving, or a strong desire or urge to use the substance.
- Social impairment:
- Failure to fulfill major role obligations at work, school, or home due to substance use.
- Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance.
- Important social, occupational, or recreational activities are given up or reduced because of substance use.
- Risky use:
- Recurrent substance use in situations in which it is physically hazardous.
- Substance use is continued despite knowledge of having a persistent or recurrent physical or psychological problem that is likely to have been caused or exacerbated by the substance.
- Pharmacological:
- Tolerance, as defined by either of the following:
- A need for markedly increased amounts of the substance to achieve intoxication or desired effect.
- Markedly diminished effect with continued use of the same amount of the substance.
- Withdrawal, as manifested by either of the following
- The characteristic withdrawal syndrome for the substance.
- The substance is taken to relieve or avoid withdrawal symptoms
- Tolerance, as defined by either of the following:
- Impaired control:
Substance-induced disorders
- Intoxication
- Substance use leads to problematic, but reversible, physiological and/or psychological changes that are specific to the substance.
- Most common behavioral changes involve disturbances of perception, wakefulness, attention, thinking, judgment, psychomotor behavior, and interpersonal behavior.
- Withdrawal
- Presents as physiological and behavioral symptoms that are secondary to a decline in blood or tissue concentrations of a substance after heavy and prolonged use.
- Substances that have a higher potential for withdrawal include:
- Substances that are rapidly and efficiently absorbed (e.g., exposure via smoking, IV, intranasal).
- Shorter-acting substances.
- Substance/ Medication-Induced Mental Disorders
- Potentially severe and usually temporary mental disorders (e.g., depression, psychosis) that develop within one month of exposure to substances, medications, or toxins or withdrawal.
- Patients must have no diagnosis of the mental disorder before the development of the mental disorder.
Likely to resolve within one month after cessation of substance intoxication/ withdrawal or medication use.
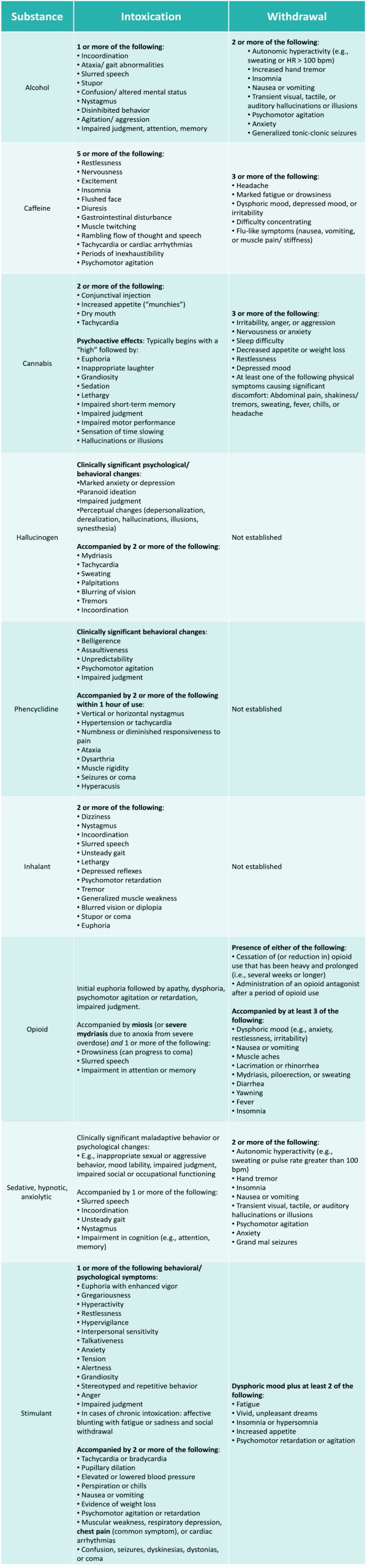
Commonly abused substances: intoxication and withdrawal symptoms
Stages of change theory
- A primary goal of psychotherapy related to substance-related disorders is to develop an action plan as individuals move through the 6 stages of change to help maintain sobriety and prevent relapse.
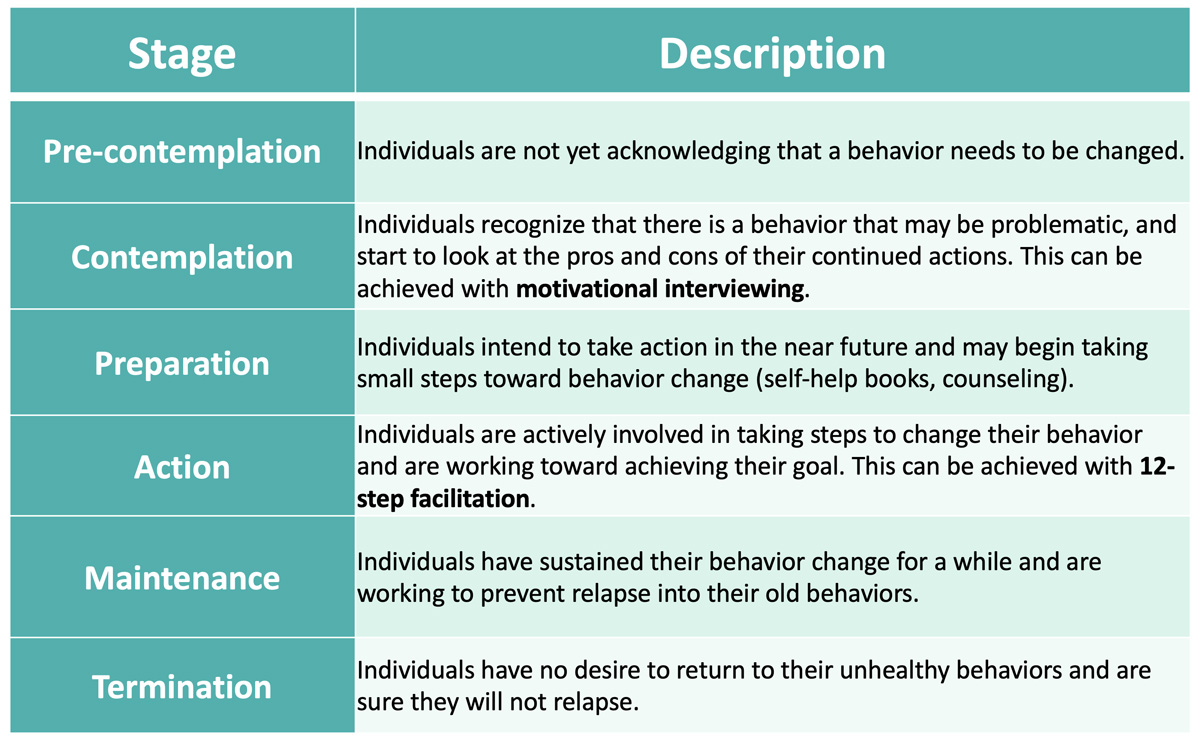
Table of Contents
[contact-form-7 id=”16199″ title=”Found an Issue? Subscriber Version”]
